
 My kid had this 24-hour-ish puke bug, and I kept anticipating that it would end sooner than it did. So, between cycles of holding back hair, wiping face, and washing out the puke pot, I thought I might be able to get this post written. Nope.
My kid had this 24-hour-ish puke bug, and I kept anticipating that it would end sooner than it did. So, between cycles of holding back hair, wiping face, and washing out the puke pot, I thought I might be able to get this post written. Nope.
I was frustrated that I couldn’t get it done, because I wanted it to be a timely dedication to a young Lymie who tragically lost her life early yesterday morning. After some reflection, I realized how selfish I was being. My daughter may be temporarily barfing up a storm, but I still have a daughter.
We have an obligation to both the living and the dead Lyme victims to expose the Lyme Crime for what it is.
If you want the senseless Lyme disease deaths to stop, you have to stop supporting ILADS now. RIGHT NOW. Do not offer prayers and condolences to the family members who are left behind, and then continue to beat the drum of “Kill the spirochetes. Kill the persisters.” That, my friends is the ultimate hypocrisy.
Who will be next? How many do we have to lose? How many mothers have to lose their babies, the light of their life, their heart and soul? Activism is nothing if it is misdirected. No, it is worse than nothing. It is devastating. It is as harmful as the Lyme scam itself. Not kidding. Not exaggerating.
Look here at what Johns Hopkins is doing.
Eradication of Biofilm-Like Microcolony Structures of Borrelia burgdorferi by Daunomycin and Daptomycin but not Mitomycin C in Combination with Doxycycline and Cefuroxime.
http://www.ncbi.nlm.nih.gov/pubmed/26903956
“Although the cause for PTLDS is unclear, one possibility is the presence of bacterial persisters not effectively cleared by the current Lyme antibiotics. Recent studies identified several drug candidates including daptomycin, daunomycin, doxorubicin, and mitomycin C that had good activity against B. burgdorferi persisters. However, their relative activities against B. burgdorferi persisters have not been evaluated under the same conditions. In this study, we tested the anti-persister activities of these drugs against both 7-day and 15-day old stationary phase cultures of B. burgdorferi individually as well as in combination with Lyme antibiotics doxycycline and cefuroxime (Ceftin). Our findings demonstrate daunomycin and daptomycin were more active than mitomycin C in single drug comparison at 10 and 20 μM, as well as in drug combinations with doxycycline and cefuroxime. In addition, daunomycin was more active than doxorubicin which correlated with their ability to stain and accumulate in B. burgdorferi. The two drug combination of doxycycline and cefuroxime was unable to eradicate biofilm-like microcolonies of B. burgdorferi persisters. However, the addition of either daunomycin or daptomycin to the doxycycline + cefuroxime combination completely eradicated the biofilm-like structures and produced no visible bacterial regrowth after 7 and 21 days, while the addition of doxorubicin was unable to prevent regrowth at either 7 or 21 day subculture.”
GREAT, right? Fantastic! They acknowledge persistent infection AND biofilms, and they offer a potential cure! Hallelujah! Praise God and ILADS for making our voices heard and advancing research!
ARE YOU ?$&@!% SERIOUS???
They have just hijacked the ILADS position, almost certainly will incorporate this “treatment” into the new IDSA guidelines, and OH YEAH: They have a new Lyme test to sell you that is no better at detecting late-stage Lyme than the existing scheme. http://jcm.asm.org/content/early/2015/10/01/JCM.02111-15.abstract
So, Magical Mystical Crystal Ball, tell me what our future holds.
The crooks co-opt the ILADS position (since they already know and have said that Lyme is a “persistent” infection–before they said it wasn’t), sell you a shiny, new treatment for your persisters and biofilms, and when you get re-tested, voila! Cured! Even though you still feel like death.
Another five years down the toilet. Another thousand (2,000? 10,000?) dead children of anguished mothers who gladly would have given their lives to save their babies. But we were so mesmerized by the Pied ILADS Pipers’ melody that we were too busy blindly following along, singing their tune, lining up for our death sentence. “So sorry for your loss.” Take a number. Get in line. March right off the cliff.
“Oh, but that can’t be true! Johns Hopkins cares! They have a new Lyme treatment clinic!”
Hopkins cares more about a chewed piece of gum stuck to the underside of a table in their cafeteria.
1.Paul Gisbert Auwaerter claims to not know what OspA is.
http://www.actionlyme.org/120420_AUWAERTER.htm
Convenient, since OspA never could have been a vaccine, and yet the crooks falsely claimed that it was, and even changed the definition of relapsing fever borreliosis to create the grand illusion that OspA indeed was a vaccine. Well, Dr. Asswaerter, your lying skills are about as sucky as that “vaccine.”
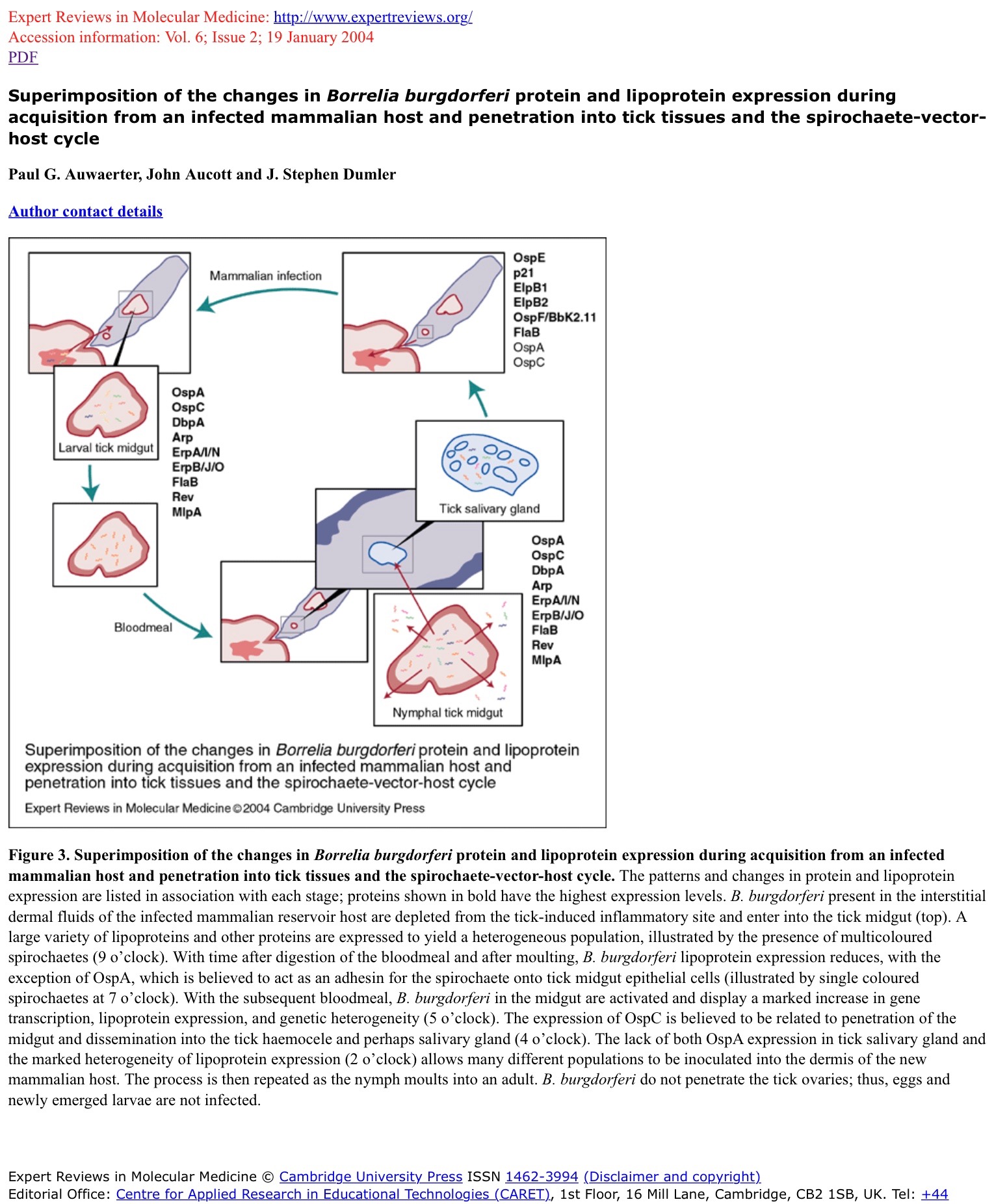
http://journals.cambridge.org/fulltext_content/ERM/ERM6_02/S1462399404007276sup006.htm
2. Auwaerter lists EBV as his number one specialty–how cute. http://www.hopkinsmedicine.org/profiles/results/directory/profile/0000525/paul-auwaerter (Of course, “PTLDS” is really chronic, active Epstein-Barr–see the Occam’s Razor–and Pauly here certainly understands. Wow, just have a look at his illustrious resume. Interesting, we’ll have to look into what he knows about measles vaccines.
3. Aucott said he needed to help Lyme victims “cope” with not having a disease.
“People with PTLDS are not hypochondriacs seeking attention or sluggards wanting to avoid work or chores, Dr. Aucott said, though they may benefit from psychotherapy that helps them cope better with their symptoms.”
When Lyme Disease Lasts and Lasts, by Jane E. Brody, July 8, 2013
http://well.blogs.nytimes.com/2013/07/08/when-lyme-disease-lasts-and-lasts/?_r=0
4. The fact that they house the Lyme clinic’s page under Rheumatology oughtta be a big red flag. http://www.hopkinsrheumatology.org/specialty-clinics/lyme-disease-clinical-research-center/
5. Give that man an award for studying the four-or-so people who tested positive and still had chronic symptoms.
“As an extension of his SLICE program at Johns Hopkins, Dr. Aucott has received a two-year grant from LRA and will recruit large numbers of patients with medically documented chronic Lyme disease.”
http://www.prweb.com/releases/2015/02/prweb12541472.htm (“Medically documented” of course means CDC two-tier positive, or arthritis-only HLAs with lots of antibodies. NOT what we victims know as “chronic Lyme.”)
6. Congratulate Aucott for being appointed Chief Dufus of the Lyme racketeers. Looks like he drew the short straw and got stuck playing the dumb but sympathetic “Lyme expert.”
“While researchers have recently given this phenomenon a medical term–Post-Treatment Lyme Disease Syndrome (PTLDS)–the exact cause of the “medically unexplained” symptoms remains a mystery. “If I knew that, I’d get the Nobel prize,” Dr. Aucott says. “That’s what our research is on, but no one knows. There’s no FDA-approved treatment for PTLDS, there’s no diagnostic test to know who’s going to get it and who isn’t. It’s pretty much a black box right now. This is a world-class dilemma. We think it is a real biological phenomenon; we just don’t know yet what it is.”
Runners and Lyme Disease, by Gretchen Voss, June 19, 2014
http://www.runnersworld.com/health/runners-and-lyme-disease
(Of course, “PTLDS” is really chronic, active Epstein-Barr–see the Occam’s Razor–and Johnny here certainly understands. But, hey, I’ll take that Nobel prize if he wants to keep playing dumb.)
7. Aucott says PTLDS patients don’t even have a real mental illness; their fatigue and depression are completely stupefying:
“No differences were found between PTLDS positive and negative groups based on demographics, prior life events, or type of coping, nor at time of diagnosis in the level of fatigue, pain, or depressive symptoms. However, immediately post-treatment, PTLDS-positive had greater depressive symptoms (mean = 9.43) than PTLDS-negative (mean = 3.98; p=0.002). At six months post-treatment, PTLDS-positive had greater fatigue (mean = 31.43) and depressive symptoms (mean = 12.00) than PTLDS-negative (fatigue mean = 16.56 p<0.001; depression mean= 1.84, p=0.012).”
https://idsa.confex.com/idsa/2012/webprogram/Paper35255.html
8. Now Aucott and his colleague Soloski are co-authors of the new Dattwyler IDSA test that’s a trick, because you only need two bands but it’s still for early Lyme only and still under 50% accurate. http://jcm.asm.org/content/early/2015/10/01/JCM.02111-15.abstract
They’re actually saying in that ^^^ report that Dearborn is not valid–therefore Klempner http://www.actionlyme.org/MKLEMPNER.htm and the “Guidelines” are false.
9. Auwaerter refers to the fake Klempner study, here, admitting that the study was not even completed. Of course, it’s even worse: two-thirds of the “retreated” patients weren’t treated a first time. http://www.acpinternist.org/archives/2007/01/lyme.htm
“IDSA’s updated guidelines were based on an evaluation of the evidence that exists from several published studies of antibiotic use for post-Lyme symptoms. According to Dr. Auwaerter, the largest and most rigorous one (a study by Klempner et al published in the New England Journal of Medicine in 2001) was stopped early because the group of patients treated with the antibiotics (parenteral ceftriaxone for one month followed by 60 days of doxycycline) were doing no better than those taking placebo pills. Whether taking antibiotics or placebo, in each group approximately one-third of patients improved, one-third stayed the same and one-third worsened.”
10. In the same article, Auwaerter advises fake treatments for your fake illness:
“Dr. Auwaerter said rather than ordering subsequent courses of antibiotics for patients with persistent symptoms, he recommends graduated, low-impact exercise and conditioning to try to build up stamina. Other options include non-steroidal anti-inflammatory agents, antidepressants, stimulants, cognitive-behavioral therapy, and psychiatric consultations. But no studies have been done studying the efficacy of these other treatment options, only of longer-term antibiotic therapy, he added.”
So, let’s step back and review:
Hopkins has for years been backing the crooks. They have supported IDSA, Dearborn and Lyme-is-an-arthritic-knee. They set up a fake Lyme clinic within their rheumatology department to prove it. They can draw diagrams of how OspA and all the other variable lipoproteins function, but they lie and say they have no idea what OspA is. They helped develop a new diagnostic test that still sucks and apparently aims to now draw a line between Lyme and CFS. They are back-pedaling on Dearborn and the IDSA (Klempner) guidelines, and now say, oh, yeah, persisters and biofilm, and here: have OUR antibiotic cocktail. CYA much?
Now who wants to believe these guys when they suddenly buy into the ILADS position on “persisters” and “biofilms,” which we know to be false, anyway?
But the bigger question remains:
WHO WANTS TO BELIEVE ILADS ANY MORE, WHEN THE FRAUDULENT, LYING, MURDEROUS IDSA CROOKS START SAYING WHAT THEY’RE SAYING?
Save a life. Denounce ILADS.
xxxxxxxxxxxxxxxxxxxxxxxxx
Dedicated to Brianna B., the latest senseless casualty in this crime beyond-epic-proportion against humanity.

Leave a reply to bloggerlenny Cancel reply