
Who woulda thought that Anthony Komaroff would spill the beans on Chronic Fatigue Syndrome just two days before CDC’s fiasco of a webinar on the next (non)generation of OspA vaccines? Add to that the CDC’s admission that Lyme is about a “damaged immune system” and the Pope mentioning fungi (see #34) in his bashing of the corporate elite polluters, and it’s been a pretty good week.
First, CDC:
Check out this USA Today article from June 16.
Paul Mead says that there may be immune system damage, a reversal of their usual line of crap, “the immune system is over-active,”since a damaged immune system would be the opposite of autoimmune (working too well):
Meanwhile, the CDC says it isn’t known why a percentage of Lyme sufferers go on to develop PTLDS, but it states on its website that most medical experts believe the culprit is a reaction produced by a patient’s own body, or “residual damage to tissues and the immune system that occurred during the infection” – not B. burgdorferi itself.
So, thanks, Dr. Mead, for catching up with your buddies over at NIH, who for years have been saying that OspA is responsible for reactivating EBV and others, via immunosuppression, resulting in MS-Lyme, Lupus-Lupus-Lyme, chronic neurological Lyme. The NIH (NINDS, actually) has a “Lyme and Multiple Sclerosis” Division (Martin and Marques). Yale used to have a “Lyme and Lupus Clinic” (now called “L2 Diagnostics”), but now they too say Lupus is most likely due to EBV. Therefore everyone agrees that OspA or the ridiculous Lyme non-vaccines were the very things responsible for the broad range of outcomes seen in Lyme.
This is the NIH (NINDS’s MS-Lyme Group) group that discovered that *** OspA *** was the cause of the MS/New Great Imitator outcome of Lyme reporting in the New York Times in the summer of 2013 (Martin and Marques, 2006):
When Lyme Disease Lasts and Lasts – Jane Brody
“Complicating the picture is the fact that some people with PTLDS symptoms apparently never had Lyme disease in the first place, Dr. Marques said in an interview. There are other infectious organisms — Epstein-Barr virus, for example — that can produce similar symptoms and may be the real culprits.”
http://well.blogs.nytimes.com/2013/07/08/when-lyme-disease-lasts-and-lasts/
Here are the NIH’s 2 reports that say OspA (TLR2/1-agonist) is the cause of the MS/CFIDS/EBV-reactivated kind of Lyme (that also causes humoral immunosuppression or NO ANTIBODIES),… and that as a result of exposure to OspA-like antigens (shed constantly in a process called blebbing, as revealed by CDC officer Alan “Stealth Bomber” Barbour), you might not even have anti-flagellar antibodies (TLR5-agonists):
Borrelia burgdorferi Induces TLR1 and TLR2 in human microglia and peripheral blood monocytes but differentially regulates HLA-class II expression.
http://www.ncbi.nlm.nih.gov/pubmed/16783164
and
Borrelia burgdorferi lipoprotein-mediated TLR2 stimulation causes the down-regulation of TLR5 in human monocytes.
http://www.ncbi.nlm.nih.gov/pubmed/16479520
Here, Mead actually says there is a real illness going on, rather than the standard Trash-the-Victim approach of calling us whack-jobs who enjoy making ourselves magically sick:
What’s more, Mead adds, because the symptoms of Lyme disease can mimic many other infections, such as the food-borne illness campylobacter and the sexually transmitted infection chlamydia, a diagnosis of “chronic” Lyme disease risks overlooking the real culprit. “In some cases, it turns out patients had an entirely different disease,” Mead says. “That’s another harmful effect … a pitfall of chronic Lyme disease diagnosis.”
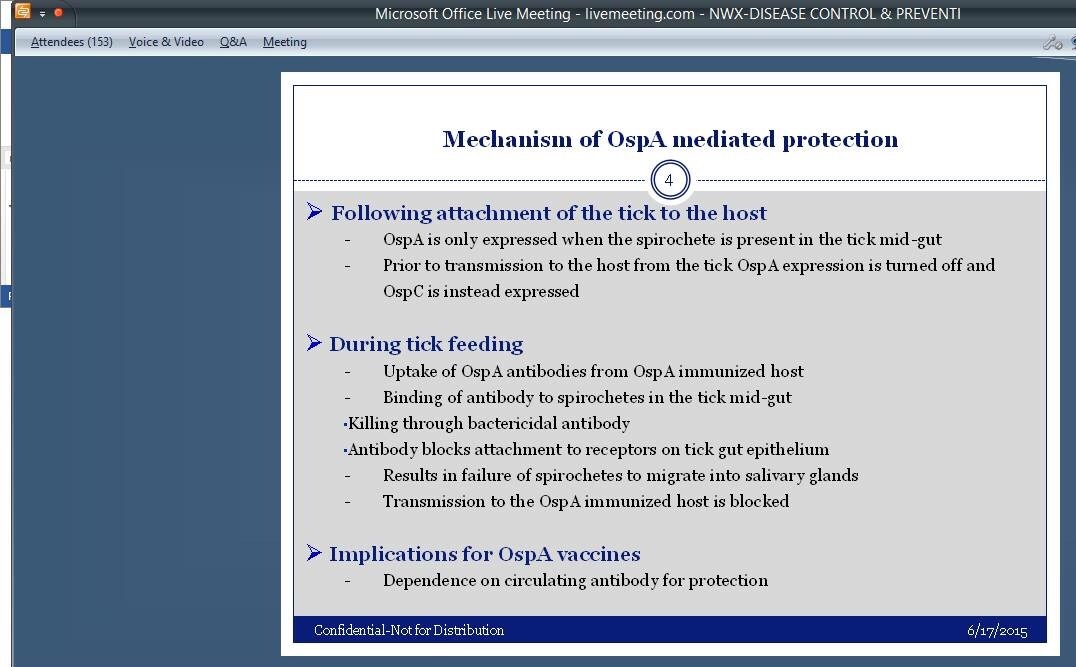
From the soon-to-be-infamous webinar–Hilarious, still insisting that OspA is immunogenic:
…When we can hop in our PubMed time machine back to 1994 and see that Fikrig reported that OspA vaccination just causes a different type of OspA and can’t be used:
Selection of Variant Borrelia burgdorferi Isolates from Mice Immunized with Outer Surface Protein A or B
: EROL FIKRIG,1* HONG TAO,2 STEPHEN W. BARTHOLD,3 AND RICHARD A. FLAVELL2,4
Infection and Immunity, May 1995
A nonclonal population of Borrelia burgdorferi N40 (passage 3) that survived protective immunity following challenge inoculation of outer surface protein (Osp) A- or B-hyperimmunized mice were characterized for the molecular basis of evasion of immunity. Two of six B. burgdorferi isolates, cultured from OspA-immunized mice, had antigenic diversity in the carboxyl terminus of OspA and did not bind to the protective OspA monoclonal antibody designated IXDII. However, OspA-immunized mice challenged with these variants were fully pro- tected. Moreover, B. burgdorferi isolates with a point mutation in ospB, which results in a truncated OspB that does not bind to protective OspB monoclonal antibody 7E6C, were frequently enriched after infection of OspB-immunized mice. These studies suggest that the incomplete efficacy of an OspA- or OspB-based vaccine may be partly due to immunomediated in vivo selective pressure, resulting in the persistence of some spiro- chetes that do not bind to protective antibodies.
Anyway, enough about those losers. When you’re dealing with criminal babies, you can only expect baby steps and denying that they have poop in their pants.
But hey–how about that Pope? (Yeah, I just segued from poop to Pope. Sorry, NQ!)
Link to his Encyclical HERE
Gotta love this quote, where he blames the capitalist scum for destroying the environment and human dignity equally well:
56. In the meantime, economic powers continue to justify the current global system where priority tends to be given to speculation and the pursuit of financial gain, which fail to take the context into account, let alone the effects on human dignity and the natural environment. Here we see how environmental deterioration and human and ethical degradation are closely linked. Many people will deny doing anything wrong because distractions constantly dull our consciousness of just how limited and finite our world really is. As a result, “whatever is fragile, like the environment, is defenceless before the interests of a deified market, which become the only rule”.[33]
Thank you, Pope Francis!
Now, about this Komaroff dude. I’m not very familiar with his past antics, having not closely followed ME/CFS politics until recently. That said, I assume he’s a bad guy in the eyes of the CFS community. For what I’m about to say, I will probably get jumped by an angry ‘tiguer in the Dollar General parking lot. I just have to point out that HE SAYS WHAT WE SAY, in this NEJM report.
First, the validation that we’re dealing with a real disease:
The Institute of Medicine (IOM) and the National Institutes of Health (NIH) recently concluded that CFS has a biological basis.2,3 Based on a survey of >9000 research articles, the IOM states that CFS “is a serious, chronic, complex systemic disease that often can profoundly affect the lives of patients.”2 Moreover, CFS “is not, as many clinicians believe, a psychological problem,”4 although some patients certainly have psychiatric comorbidities requiring diagnosis and treatment.
Next, neurological abnormalities (indicating infections in the CNS, thank you very much):
Many objective, measurable differences distinguish patients with CFS from healthy individuals or patients with other fatiguing illnesses (ranging from major depression to multiple sclerosis).5 Cognitive studies reveal slowed information processing and deficits of attention and memory in patients with CFS, and functional MRI shows that cognitive tasks require recruitment of more areas of the brain. Standard MRI studies point to white matter abnormalities and decreased gray matter volume. Encephalographic analyses have distinguished unmedicated CFS patients from healthy individuals and from patients with major depression.
The IOM has concluded that the hypothalamic-pituitary-adrenal axis (and possibly several other neuroendocrine axes) is disordered. Compared with healthy individuals and patients with major depression, CFS patients have lower levels of overnight cortisol, 24-hour urinary cortisol, corticotropin-releasing hormone or arginine vasopressin (or both), and adrenocorticotropin hormone. Defects in the autonomic nervous system are clinically manifested by orthostatic intolerance (heart rate and blood pressure abnormalities when standing or during head-up tilt testing).2
And here you go. The part where he actually describes what post-sepsis syndrome is:
Many patients with CFS have poorly functioning NK cells (a lymphocyte subset that defends against viral infections and malignancy) as well as altered blood levels of various cytokines.2 In a study of 298 CFS cases compared with 348 healthy controls, analysis of 51 different cytokines and related analytes suggests that CFS is driven by an immune system that is chronically activated for several years following onset and then perhaps “exhausted” from this chronic activation as the duration of the illness lengthens.6
These results are provocative because the symptoms of CFS could well reflect cytokine production in the brain from a neuroinflammatory process. Indeed, a positron emission tomography study demonstrated brain neuroinflammation (activated microglia or astrocytes) in patients with CFS.7 Moreover, when cytokines are given therapeutically (e.g., interferon for hepatitis B and C), the infusion often produces fatigue and other CFS-like symptoms.
Then, as if that didn’t just feel like Christmas morning, he whips out the old Epstein-Barr Virus, along with our favorite, FUNGI, and some other gunk, before again emphasizing chronic infections of the brain:
CFS can follow infection with Epstein-Barr virus (and possibly other specific viral, bacterial, and perhaps protozoal infections).2 However, no infectious agent has been proven to cause the ongoing symptoms of CFS — and a single, novel infectious cause is unlikely to explain most cases. It is plausible (but unproven) that a significant proportion of cases are triggered and perpetuated by any of several chronic infections of the brain and infection of immune cells associated with peripheral nerves.
I will leave you with two final kickers from Komaroff.
1. Your depression is not causing your illness. Your illness is pissing you off and the stupidity of the medical profession is what’s depressing:
In contrast to people with major depression, patients with CFS generally do not appear downcast or express feelings of hopelessness and helplessness or describe anhedonia. The exceptions are those suffering from both CFS and a secondary (reactive) depression.
2. A little exercise’ll do ya, maybe, but don’t let it do ya in.
The AHRQ report concluded that counseling therapies and graded exercise therapy help improve fatigue and function in some patients. These approaches are not curative, and exercise therapy must be pursued very cautiously as it led to more adverse events and withdrawals in several trials.
Thank you, Dr. Komaroff for such a fascinating and enlightening lesson in Toldya So.

Leave a reply to The Other Side Of The Stretcher Cancel reply