The Beginning and the End
Remember when you were a kid, and you had your favorite “sick food?” Mine was toast with butter and honey, but the butter had to be completely melted so the honey could fully penetrate the toasty crevices. Do you have someone to make honey toast for you when you get sick now, as a grown-up?
If you got sick, would someone be there to watch TV with you and tell you, “Nah, you don’t stink at all”? If you stayed sick, would someone be there to take you to doctors’ appointments, pick up your meds from the pharmacy, tidy up your house? If you got really sick, would someone be there to make sure you’re eating, offer to take care of your kids and pets?
What if you were so sick you could no longer work or take care of yourself? Would someone be there to provide support—emotional, financial, or otherwise?
It is said that most deaths from Lyme disease occur as a result of suicide. Of course, we have no real statistics, because, if you can’t get diagnosed in the first place, how can your suicide be attributed to Lyme?
Did you know that the CDC now acknowledges that there are about 300,000 new cases of Lyme disease every year in the United States? Did you know this figure is six times higher than HIV/AIDS, yet only about 10% of the Lyme cases are allowed diagnosis and treatment?
The other 90%? They’re written off as crazy or lazy and abandoned by their family and friends—those who should be first in line to show them compassion and love.
Why? I’m at a loss. Trying to make sense of what motivates people to be abandon others in their time of greatest need—when their health has completely failed them—is like trying to understand how 2+2 can equal 5. Yet, this is reality for many with whom I come into contact every day. It’s a reality that has devastating consequences.
No Diagnosis, No Dice
 People who can’t get a diagnosis (and I mean ANY diagnosis, LET ALONE Lyme) and who live in excruciating pain and sickness every day, are treated like frauds by most doctors. Where does that leave a person? You can’t get pain meds—they’ve pretty much outlawed them at this point. (They’d love to give you psych meds, though.) Family, friends, employers, complete strangers…nobody seems to understand that yes, it is possible to be impossibly sick, and no, we would not choose to be sick if the option existed.
People who can’t get a diagnosis (and I mean ANY diagnosis, LET ALONE Lyme) and who live in excruciating pain and sickness every day, are treated like frauds by most doctors. Where does that leave a person? You can’t get pain meds—they’ve pretty much outlawed them at this point. (They’d love to give you psych meds, though.) Family, friends, employers, complete strangers…nobody seems to understand that yes, it is possible to be impossibly sick, and no, we would not choose to be sick if the option existed.
The truth is that most Lymies are walking around with an AIDS-like disease, pretending with all their heart to be functional, while fully knowing that on the inside, everything is disintegrating into a puddle of useless sludge. They are barely hanging on, working to support a family, pay the mortgage, cover medical bills that are denied by insurance, put on a show of everything’s-rainbows-and-unicorns, all while harboring this AIDS-like disease that is killing them from the top down, from the inside out.
And at some point—maybe when the bills become too much to take, maybe when a sentence can no longer be strung together, maybe when the agony of getting out of bed and facing another stressful day of working while disabled—people crack. Suicide does become the only option. AIDS patients, in the beginning, had the luxury of death. Lyme victims are subjected to an inhumane and never-ending torture of body, mind and spirit.
Those are the ones who are still standing. Countless others are homebound, bed bound, and quite frankly don’t have the strength or means to commit the unthinkable. Still, they find a way.
We Need Compassion, and Other Stuff
Where is the compassion? We are too sick and poor to organize and protest. Besides, who would we protest? This criminal conduct which rules Lyme policy runs the gamut from academia to medical associations to government. Are we supposed to say, “Please, criminals, stop torturing us?” We are not a protected class; this disease affects all races, religions, genders and ages. We are shunned and blackballed by doctors who determine us to be “difficult” or “non-compliant.” Then, adding insult to injury, we’re abandoned by family and friends—why? This, I do not understand. WHY? Why would a human being dump another human being like the scraps off their dinner plate, into the disposal?
We cannot get disability unless we are “lucky” enough to get a diagnosis of one of the serious outcomes of chronic Lyme: MS, ALS, Alzheimer’s, Cancer. Even then, we’re told, “See? It wasn’t Lyme after all.” The media will only cover the “fluff” of personal stories, and not the real reason we are in this unfathomable situation. “We need more research! We need more antibiotics! We need bills to protect doctors,” go the chants. NO. That is not what we need.
We need healthy human beings to open their eyes, understand the facts and grasp the truth. Please. It is not beneath us to beg. We are already at rock bottom.
The Testing: An Introduction
According to the Centers for Disease Control (CDC), an estimated 300,000 people per year contract Lyme disease in the U.S. (1). That makes Lyme six times more prevalent than HIV/AIDS (2), yet HIV funding eclipses that of Lyme disease by nearly 135 times (3).
Family, friends, employers, doctors, everyone…we need you to understand WHY Lyme cases are vastly underreported. The only diagnostic test endorsed by the CDC is known as the “two-tier” protocol, or the “Dearborn standard” depending on who you ask. Basically, if you go to a doctor with a known tick bite or a bulls-eye rash, you might be lucky enough to be identified as a potential Lyme case.
On the off-chance that actually happens, the doctor would likely take one of these actions:
- In extremely rare cases, he might prescribe two or three weeks of doxycycline, the standard antibiotic treatment for suspected early cases of Lyme.
- In some cases, he might prescribe a single “prophylactic” dose, which is woefully inadequate for eradicating the infection even if it is caught early.
- In most cases, the doctor will either deny that Lyme is a possibility or opt for a “wait and see” approach. This is a self-fulfilling prophecy, as you will see by reading on. Actual cases go undiagnosed, leading to the false belief that Lyme disease is rare, and in some places thought to be non-existent.
Now, let’s take a closer look at the possibility that the doctor might actually decide to run some tests. That’s where the “two-tier” test comes into play.
Tier one is called an Enzyme Linked Immunosorbent Assay (ELISA). The ELISA looks for non-specific antibodies in the blood. It’s supposed to be a “screening” test, and if the patient produces enough antibodies, he or she wins the jackpot and gets the opportunity to have a Western blot done—the second tier of testing.
Tier two, the Western blot, is designed to identify specific anti-borrelial antibodies in the blood. The CDC’s surveillance criteria, which they state are NOT supposed to be used for diagnosis, require two out of three specific IgM (acute infection) antibodies or five out of 10 specific IgG (past infection) antibodies. But doctors use the surveillance criteria for diagnosis, anyway, and end up thinking that actual Lyme cases are very rare. Need I state that with an AIDS-like disease, “immune deficiency” means that a person lacks antibodies?
Am I making myself clear? This disease is like AIDS, but the only tests used to diagnose it do not work, and doctors are trained to look away—nothing to see here. That leads to accusations of fakery, hypochondria, and ultimately, abandonment by family and friends. And the most horrific pain, anguish, loneliness and despair that you can imagine. Depression. Suicide. Would someone be there for you? Would you be there for someone? I’m sure my dear readers would make the right choice. Right? Make the honey toast. Then go a step further.
Consider the Part About the Fraud
The two-tier test protocol is a fraud.
The ELISA was designed to detect only HLA-linked (genetically predisposed) arthritis, or hypersensitivity, cases, which account for about 15% of all cases. Where does that leave the other 85% who don’t have arthritis? You guessed it: they are the ones with an AIDS-like disease. How do we know this?
When certain CDC officers saw the potential market size for drugs and diagnostics (look, ma—300,000 per year!), they decided to do some product development. That involved coming up with a vaccine, even though, at that time, it was well known that Lyme disease is actually a “relapsing fever,” making a vaccine impossible. The nature of relapse is such that the borrelia organism—a spirochete, which is not a bacteria, but its own phylum—undergoes antigenic variation, or the ability to change the expression of its outer surface proteins and “bleb” or shed them to evade the host’s immune response.
If the organism is constantly changing and shedding its outer surface proteins, it is a moving target for the immune system. This is why a vaccine is not possible. This cabal who decided it would be a great idea to make a Lyme vaccine also thought it would be brilliant to select just one of those outer surface proteins, Outer Surface Protein A (“OspA”) to use as the antigen in the LYMErix vaccine.
Unfortunately, OspA is the very antigen that is responsible for the AIDS-like illness in 85% of its victims. But, no worries: there was a plan to fix that little marketing problem.
How it All Went Down
During the late 1980s to early 1990s, the bar for getting a diagnosis was much lower, and was based (correctly) on Lyme being a relapsing fever organism. The CDC’s own diagnostic standard of performing repeat Western blots to look for new IgM bands was due to the knowledge that not all spirochetes would be killed by antibiotics, and new bands would appear as a result of new antigens being produced by the spirochetes. This came out of CDC officer Allen Steere’s own, 1986, published observations of the serology over time.
In 1992-93 Steere, while on the SmithKline payroll for LYMErix trials, falsified this case definition such as to say, “No longer do you need repeat Western blots to look for new IgM bands; you instead need to have several late Lyme arthritis bands (HLA-linked hypersensitivity or allergy)”—excluding all of the neurologic cases, which he knew to be the most serious outcomes of Lyme.
He published two important reports, neither of which is available free, full-text online:
- “Western blotting in the serodiagnosis of Lyme disease” (included in the CDC’s Dearborn booklet)
- “Antibody responses to the three genomic groups of Borrelia burgdorferi in European Lyme borreliosis” (not included in the CDC’s Dearborn booklet)
The first one was included in the booklet from the CDC’s 1994 conference in Dearborn, Michigan, which has come to be known simply as “Dearborn.” The second report was not included. I’ll get into that after a brief explanation of Dearborn.
 The Dearborn conference was presented as a meeting to standardize the method of diagnosing Lyme, but what it became was a farce in which those involved in the LYMErix scam—CDC officers—pushed through a new method of interpreting the testing. By doing so, they effectively changed the definition of Lyme disease from relapsing fever neurologic disease to a disease of an arthritic knee. It is no surprise that the labs that participated did not agree with the “consensus” recommendation, nor is it a coincidence that they had an average accuracy rate of 15% with the new method.
The Dearborn conference was presented as a meeting to standardize the method of diagnosing Lyme, but what it became was a farce in which those involved in the LYMErix scam—CDC officers—pushed through a new method of interpreting the testing. By doing so, they effectively changed the definition of Lyme disease from relapsing fever neurologic disease to a disease of an arthritic knee. It is no surprise that the labs that participated did not agree with the “consensus” recommendation, nor is it a coincidence that they had an average accuracy rate of 15% with the new method.
Back to the reports: Why is only the first Steere report included in the Dearborn booklet? Because the second one, “…European Lyme borreliosis,” reveals how Steere committed research fraud to falsify the current case definition, leaving OspA and B out of the antibody testing. (OspA and B are encoded on the same short section of free floating DNA called “plasmids,” so you can’t leave out one without the other).
He did this by using high-passage strains, which drop plasmids, and by using recombinant OspA and B proteins without the tri-palmitoyl group (the 3 fatty acids), which are necessary to produce antibodies. The result was that OspA and B were fraudulently missing from the Dearborn diagnostic panel.
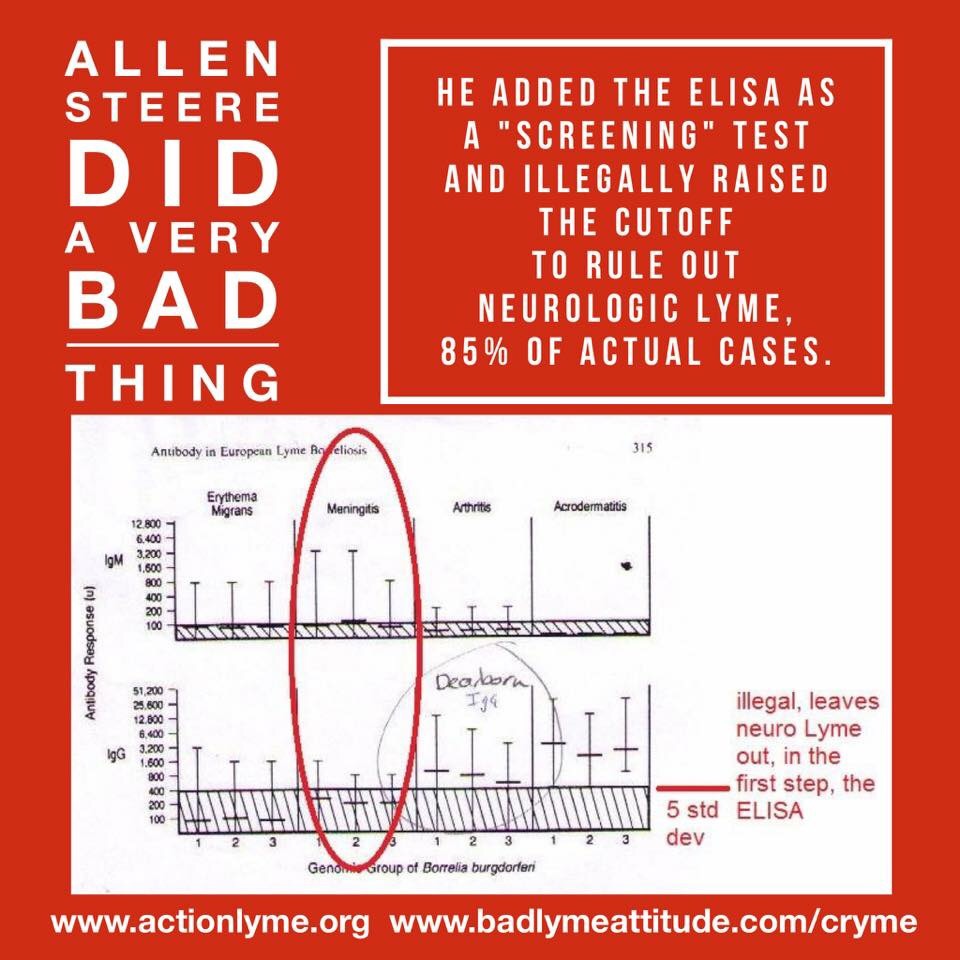 Additionally, Steere proposed adding the first-tier ELISA, while he knew that neurologic Lyme was mostly antibody-negative since he had published about it in 1990. He used the Volkman-Dattwyler “seronegative Lyme assay” (which looks for cellular rather than humoral immunity), and arbitrarily raised the cut-off for the ELISA to exclude all neurologic cases.
Additionally, Steere proposed adding the first-tier ELISA, while he knew that neurologic Lyme was mostly antibody-negative since he had published about it in 1990. He used the Volkman-Dattwyler “seronegative Lyme assay” (which looks for cellular rather than humoral immunity), and arbitrarily raised the cut-off for the ELISA to exclude all neurologic cases.
Welcome to Starship Lyme Enterprise: Motive
To summarize Steere’s shenanigans, he falsified the case definition for Lyme, leaving out OspA and OspB, known to be “primary immunodominant antigens,” and artificially raised the cutoff on the ELISA (ruling out neurologic cases), and did so because:
- You never test for a disease with the same antigens as the vaccine. If 85% of cases could no longer be detected, the vaccine would be declared “safe” in trials.
- If it was known that borreliosis and other fungal-antigen-laden tick-borne infections were mostly antibody-negative, everyone would know that the vaccines and test kits were useless, and
- What was to happen after an OspA vaccine was on the market—a monopoly on all vector-borne diseases testing, blood and DNA opportunities in the blood, such as HLAs (“ethnic bioweapons”), and new test kits and vaccines for all the new diseases to come along (such as babesia, new borrelia, viruses, fungi, etc.).
All of this—getting a fake vaccine out there—was for the intended LATER monopoly on American and Canadian blood testing for all vector borne diseases. It was a whole new genre of vaccines profiteering. All of it was to be owned by the RICO enterprise originally headquartered at New York Medical College, called the American Lyme Disease Foundation (ALDF.com).
They even called themselves an “enterprise” (Arthur Weinstein) and said that tick-borne disease $$$ opportunitie$ were “a rich vein of gold from which to mine virulence determinants” (CDC officer Alan Barbour).
Consensus or not, we were force-fed this change at Dearborn, and LYMErix was full steam ahead. The vaccine trials were declared a success—85% effective!—and LYMErix hit the market in 1998.
It didn’t take long before adverse event reports started rolling in with horrifying stories of disablement. There were government hearings; a whistleblower presented evidence of OspA being a toxin; and the FDA issued an ultimatum: either pull the vaccine from the market or we will. The manufacturer did, and LYMErix went down in history as having been discontinued due to low sales. Thanks a lot, FDA.
And to this day, kids, we are left with a bogus disease definition, a government-endorsed diagnostic protocol that misses 85% of cases, and a medical system that is rotten to the core for its abuse of victims of AIDS 2.0. The end.
But it Doesn’t Have To Be The End.
Doctors can start treating people with dignity and respect, instead of accusations and belittlement. Family members can start offering help without questioning motives. Friends can employ a “willing suspension of disbelief” just long enough to see the suffering that is going on beneath the spit-shined exterior. Open your mind and your heart to someone who has reached rock bottom, and offer a hand up. We bottom-dwellers are prone to forgetting sometimes that “up” still exists.
Make the Honey Toast.
Helping Lyme sufferers on a personal level will go a long way toward making life worth living, but we also need two things to happen at the federal level.
We need this fraud prosecuted by the United States Department of Justice. A complaint was filed in 2003 with all the pertinent information—everything necessary to prove the crime and its outcome. But here we are, 12 years later, with nothing. No response, no movement, no people getting any better. Three hundred thousand new cases per year. Conservatively.
We believe that with prosecution of the fraud, the door will be opened to research into treatments that are appropriate for an illness that is in the AIDS and cancer class.
Along with prosecution of the fraud, we need the FDA to invalidate the existing testing scheme. Remember that without an accurate test, the sickest 85% of Lyme patients are denied diagnosis, care, compassion, proper treatment, insurance coverage, and even disability insurance, even though they are disabled and can’t (or shouldn’t) work. This is an easy thing for the FDA to do. It need only follow its own rules for the validation of an analytical method—using the real disease definition of relapsing fever borreliosis—to see that Steere’s test method is a fraud.
Once these things happen, Yale University’s involvement will be exposed, along with the only truly valid (by FDA standards) test method in existence, which Yale researchers patented. If you’re interested, look up U.S. patent 5,618,533; they’ve been sitting on it, knowing full well how badly it is needed.
Once all the Lyme crimes are prosecuted and the crime scene cleaned up, then we can get to the business of treating people for what the disease truly is. I keep throwing “AIDS-like” around. I don’t do that to be dramatic. The fact is, there are many, many sources of peer-reviewed research that support this description of Lyme disease. I’ve provided some of these links below.
If you are healthy, or have an arthritic knee, consider yourself blessed. Those of us in the trenches of the Lyme wars are getting weary. We are sick, and yet we go on—what else can we do? I can’t bear the thought of the alternative any longer. Let me be clear: It is NOT okay that people feel they have no choice but to end it all.
If you are healthy, won’t you help us? Will you speak for us when we can’t find the words? Will you stand for us when we don’t have the strength? Will you tell our story as if it were your own? Will you join our ranks before you are forced by Lyme disease to join us anyway?
We have learned the utmost compassion through this journey, and we promise to be there for you when we are able. Toast, or whatever.
- http://www.cdc.gov/media/releases/2013/p0819-lyme-disease.html
- http://www.cdc.gov/hiv/statistics/basics/ataglance.html
- http://report.nih.gov/categorical_spending.aspx
For a downloadable pdf of the complete Lyme Cryme charge sheets, click Charge Sheets
Links to studies from scientists who know what they are talking about regarding Lyme/OspA immunosuppression:
“Endotoxin tolerance is thought to limit the excessive cytokine storm and prevent tissue damage during sepsis but renders the host immunocompromised and susceptible to secondary infections.”
http://www.ncbi.nlm.nih.gov/pubmed/23695305
http://www.ncbi.nlm.nih.gov/pubmed/?term=Redmond+HP+and+tlr2
http://www.ncbi.nlm.nih.gov/pubmed/?term=Baumgarth+and+borrelia
http://www.ncbi.nlm.nih.gov/pubmed/?term=Barthold+and+borrelia
http://www.ncbi.nlm.nih.gov/pubmed/?term=Martin+and+Marques+and+tlr2 (
http://www.ncbi.nlm.nih.gov/pubmed/?term=Harding+CV+and+tlr2
http://www.ncbi.nlm.nih.gov/pubmed/?term=Medvedev+AE+and+tlr2
http://www.ncbi.nlm.nih.gov/pubmed/?term=Hotchkiss+RS%5BAuthor%5D
http://www.ncbi.nlm.nih.gov/pubmed/?term=Duray+and+borrelia
http://www.ncbi.nlm.nih.gov/pubmed/?term=Dattwyler+and+borrelia+and+nk+cells
Benach: Borrelia wreck your brain:
http://www.ncbi.nlm.nih.gov/pubmed/?term=Benach+and+borrelia
Cadavid: Borrelia wreck your brain:
http://www.ncbi.nlm.nih.gov/pubmed/?term=Cadavid+and+borrelia+and+brain
Gary Wormser on how the OspA vaccines in dogs didn’t work and caused immunosuppression:
http://www.ncbi.nlm.nih.gov/pubmed/10865170
Latov on how OspA vaccination caused the same disease as chronic Lyme:
http://www.ncbi.nlm.nih.gov/pubmed/15363064
Marks on how LYMErix caused the same disease as chronic Lyme:
http://www.ncbi.nlm.nih.gov/pubmed/21673416
Mario Philipp on how Lyme and OspA causes immunosuppression with brain inflammation:
http://www.ncbi.nlm.nih.gov/pubmed/?term=Philipp+M+and++tlr2

Leave a reply to Help Wanted: Lyme – AIDS 2.0 | Slices Of Lyme Pie Cancel reply