
Lyme brothers and sisters, I want to empower you, but this won’t be easy. Fair warning.
I had a really crappy job for six years. Part of what made it so bad was the lack of communication, lack of accountability and lack of balls when difficult news needed to be shared. Everything was lied about, hidden or sugar-coated. The company’s leaders promoted a culture of disrespect, in which we plebes weren’t good enough or smart enough to handle the truth.
It’s the same way with Lyme. Go to just about any “support group” or nonprofit Website and you can experience this culture, where those in power decide what the truth is, and what you’re capable of handling intellectually and emotionally.
At work we got a new vice president who promoted open communication. We were forced to read a cheesy book about giving and receiving feedback. It said that the type of feedback that is the honest truth but a bitch for the receiver to handle and accept, is called a “gut punch.” It’s the kind of feedback that you don’t want to hear, but need to hear.
Here is the painful but empowering Lyme gut punch:
“Chronic Lyme disease” is a misnomer. The crooks were right. You don’t have Lyme disease.
Now, before everyone starts composing their nastygrams, hear me out, and consider whom you should send them to. Hint: it’s not me.
“Lyme disease” as defined at the CDC’s 1994 Dearborn conference, is an arthritic knee hyper-sensitivity response–lots of antibodies scurrying off to do battle. What chronic Lyme sufferers have is the opposite–sub-immune. No antibodies doing anything. Post-sepsis. Immune paralysis. Acquired immune deficiency. At Dearborn they redefined the disease to exclude our cases because the vaccine, LYMErix, caused the same disease.
“But I didn’t get the vaccine, so it doesn’t matter.”
To be clear, the antigen in the vaccine, Pam3Cys (the same poison as OspA from Lyme spirochetes), caused “chronic neuro-Lyme” just as if it had been injected by a tick.
Let that sink in.
…
…
…
…
…
Pam3Cys, or OspA is the cause of “chronic Lyme disease.” Pam3Cys was injected by syringe–no spirochetes, no coinfections.
That means ticks are not necessary to cause Lyme disease.
Spirochetes are not even necessary.
All you need is something like E. Coli poop toxin (well known for eons as a sepsis-inducing poison), such as Pam3Cys/OspA.
ILADS has fooled everyone into becoming spirochete killing machines, when it has been known practically forever that you can’t kill those buggers, and they’re not really to blame, anyway. In fact, blaming the spirochetes is like shooting the messenger, kinda like when you get one of those “gut punches” and lash out at the person delivering the message.
So, if ticks and spirochetes aren’t necessary to cause “chronic Lyme,” guess what else they make unnecessary?
Busting biofilms. Blasting cyst forms. Paying ILADS. All of the “nonprofit” advocacy groups. All unnecessary.
This is not a bacterial disease. It’s a nightmare of immunological meltdown.
This is what Pam3Cys/OspA looks like, chemically speaking. (This section credit to Kathleen Dickson, ActionLyme.org)
“What is variable is the protein end “(“peptide”), but what is immunogenic (seen as an invader to the immune system) are the fatty acids or acyl groups and the very electronegative cysteine core”:
“Pam3Cys is a triacylated lipoprotein, the degree of acylation is equated with its toxicity. So what is acylation? It’s the zig-zaggy lines that mean Carbon-Carbon-Carbon, yes, hydrocarbons, like margarine or octane. The name just refers to the number of carbons in each carboxyl or acyl group. Palmitic (the Pam in Pam3Cys) has X number of carbons, gasoline, 8, linoleic acids, like 14. Look up what are alkanes then add a COOH group and you have one of these fatty acids.Something highly acylated like this (3 or more fatty acids hanging off) are managed by Toll-like Receptor (TLR) 2 and TLR1, together. Therefore a “TLR2/1-agonist” is another term that generally refers to lipoproteins like those from Borrelia, mycoplasma, mycobacteria, and others, like Brucella. (But they can manage other compounds.)”
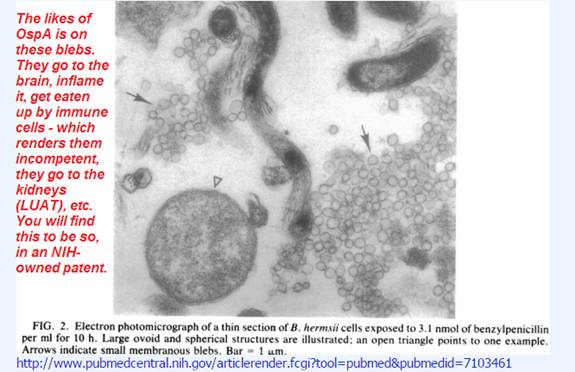
This thing, Pam3Cys and fungal lipid molecules like it, is shed with the blebs. In other words, like this:
The likes of OspA is on these blebs. They go to the brain, inflame it, get eaten up by immune cells – which renders them incompetent-, they go to the kidneys (LUAT), etc. You will find this to be so in an NIH-owned patent (5,217,872) and elsewhere.So, the fungal antigens are on the shed blebs and they go everywhere and they render the immune cells incompetent, resulting in an AIDS-like disease. Everyone who has Lyme disease also has LYMErix disease.”
(Thanks, Kathleen.)
Further to the point about Pam3Cys (LYMErix) and OspA (tick sepsis antigen) being the same thing and being THE cause of “chronic Lyme disease,” here is the Mayo patent (filed in 1996) for distinguishing B. Burgdorferi infection from OspA vaccination:
Inventors: Persing; David H. (Rochester, MN)
Assignee: Mayo Foundation for Medical Educational Research (Rochester, MN)
Family ID: 24452298
Appl. No.: 08/612,231
Filed: March 7, 1996
Method for detecting B. burgdorferi infection
http://patft1.uspto.gov/netacgi/nph-Parser?Sect1=PTO1&Sect2=HITOFF&d=PALL&p=1&u=/netahtml/PTO/srchnum.htm&r=1&f=G&l=50&s1=6045804.PN.&OS=PN/6045804&RS=PN/6045804
Abstract
The present invention provides a method for detecting B. burgdorferi infection utilizing an antigen preparation lacking a detectable level of outer surface protein A (OspA). The antigen preparation is made from an isolate of B. burgdorferi that lacks the plasmid encoding outer surface protein A (OspA). The method of the invention discriminates B. burgdorferi infection from OspA vaccination.
Think about it. Why would you need a test to tell the difference unless they were the exact same disease?
Recap: There is “Lyme disease,” AKA the Dearborn case definition that we’re always trying to achieve on a Western blot; then there is *our* disease of post-sepsis from the injection of a fungalish, poopish toxin, OspA/Pam3Cys. In all but a few outlier cases, if you are CDC-positive, you’re not really sick. So quit trying to be CDC-positive. You’ll ruin your credibility as a sick person.
If you’re in this boat– the post-sepsis sh!t-show one– with the millions of us who feel as if we’re bailing water from the Titanic with a teaspoon, guess what? There are gobs of scientists who will validate your illness without trying to sell you ridiculous treatments or get you to take another tiresome survey about your tiresome symptoms.
Richard Hotchkiss of Washington University in St. Louis is one. He has published extensively about the permanent immune system damage that causes long-term illness after sepsis.
The new normal: immunomodulatory agents against sepsis immune suppression
Noelle A. Hutchins, Jacqueline Unsinger, Richard S. Hotchkiss, Alfred Ayala. Trends in Molecular Medicine, http://www.cell.com/trends/molecular-medicine/issue?pii=S1471-4914(14)X0003-1
http://www.ncbi.nlm.nih.gov/pubmed/24485901
“Sepsis is the leading cause of death among critically ill patients in intensive care units, and treatment options are limited. Therapies developed against the proinflammatory stage have failed clinically; therefore, new approaches that target the host immune response in sepsis are necessary. Increasing evidence suggests that ***a major pathophysiological event in sepsis is immune suppression, often resulting in secondary fungal, bacterial, or viral infections.”***
Alan Barbour (CDC, IDSA) recently was editor on a UCSF study that demonstrated nearly half of cases remained sick despite antibiotic treatment–supporting the notion that damage is done to the immune system very early in the disease process, and it’s not about spirochetes.
“Six months after completion of therapy, Lyme disease patients were found to have 31 to 60% of their pathways in common with three different immune-mediated chronic diseases. No differential gene expression signature was observed between Lyme disease patients with resolved illness to those with persistent symptoms at six months post-treatment.
Six months after treatment, 15 of the 29 patients in the study had fully recovered, while 13 had persistent symptoms, and one had dropped out. Despite the stark differences in how the patients reported feeling, the researchers could not detect transcriptional differences between the two groups. They said larger studies are needed to confirm this finding.”
Curious, isn’t it, that this study comes 27 years after IDSA first pointed out that treatment fails in half the cases?
perspective on the treatment of Lyme borreliosis.
Rev Infect Dis. 1989 Sep-Oct;11 Suppl 6:S1518-25. Review.
PMID: 2682965 [PubMed – indexed for MEDLINE]
Luft BJ, Gorevic PD, Halperin JJ, Volkman DJ, Dattwyler RJ.
The UCSF report also said:
“Early Lyme disease prior to antibiotic therapy was characterized by marked upregulation of Toll-like receptor signaling but lack of activation of the inflammatory T-cell apoptotic and B-cell developmental pathways seen in other acute infectious syndromes.”
(That means immunosuppression, kids.)
Another scientist who gets it is Nicole Baumgarth of UC Davis. She and her team described the immunosuppression caused by OspA and its spread to immune receptors that handle viruses, such as the flu.
http://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1004976
Suppression of Long-Lived Humoral Immunity Following Borrelia burgdorferi Infection
Rebecca A. Elsner, Christine J. Hastey, Kimberly J. Olsen, Nicole Baumgarth
Published: July 2, 2015http://dx.doi.org/10.1371/journal.ppat.1004976
“Infections with the Lyme Disease agent, Borrelia burgdorferi, often fail to generate long-term protective immunity. We show here that this is because the immune system of the Borrelia-infected host generates only short-lived, structurally abnormal and non-functional germinal centers. These germinal centers fail to induce memory B cells and long-lived antibody-producing plasma cells, leaving the host susceptible to reinfection with Bb. This inability to induce long-term immunity was not due to the nature of Borrelia antigens, as even T-dependent antigens of Borrelia were unable to induce such responses. Moreover, influenza vaccine antigens, when applied during Borrelia-infection, failed to induce strong antibody responses and immune-protection from influenza challenge. This data illustrate the potent, if temporal, immune suppression induced by Borrelia-infection. Collectively, the data reveal a new mechanism by which B. burgdorferi subverts the adaptive immune response.”
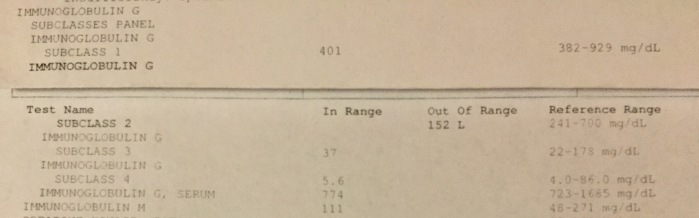
Now, because we Lymies inevitably want to see anecdotal evidence, I’m going to humor you for a moment. Here is a real-life example of the immunosuppression that I’m talking about. This first image is my Immunoglobulin G panel from 5-1/2 years ago.
Notice that my Subclass 2 was deficient, but my total IgG was still within the reference range.
The second image is from this year.

Notice, first of all, that the reference range for total IgG is now lower than it was six years ago. They’ve changed the standard for immune deficiency, making it “normal” to have a crappy immune system. Second, they don’t like to test the four subclasses because that would reveal more than the insurance industry would like to deal with, like the probability that all of my subclasses have tanked, since they were teetering on the edge before.
Despite the goalposts being moved, I got sicker, faster than the average that they use to set the bar, going from 774 to 680 to achieve official “immune deficient” status. And my IgM is nothing to write home about, either. Immunologists pretend that this is all genetic, and we’re programmed to self-destruct at a genetically pre-determined age. They don’t care to understand the pathogenesis of immune deficiency–and why would they? It’s easy and profitable to prescribe IVIG and a load of other pharmaceutical symptom-obscurers.
What does this mean to the average Lymie? Well, compared to a lot of those I run into online, I’m doing pretty well. Just imagine what these numbers would look like for someone who is bed-bound. Not pretty. So how about you ask your famous ILADS doctor to run an IgG subclass panel? What will he say? Will he claim to be able to fix it? Can he cure you?
If so, he is a fraud and you need to fire him. This is not fixable with antibiotics, “biofilm busters,” supplements, herbs, rife, ozone, onion socks, Horrorwitz’s latest book, etc. It’s a B-cell disease similar to lymphoma. Post-sepsis. Immune paralysis. Acquired immune deficiency. What’s the treatment? Probably something similar to a cancer treatment. Because I’m not a *doctor*, I’m not qualified to provide treatment advice. Unfortunately, neither are any of the licensed MDs. There’s not a single MD anywhere who is both eligible to provide, and capable of providing, such advice. They don’t do science.
ILADS won’t talk about any of this. LDA, Lymediseasedotorg and other nonprofits who claim to be fighting for us shut down any conversation about the fraudulent testing and instead focus on research into biofilms and persisters, or surveys about how badly your symptoms suck.
They all need to be called out for their ongoing obstruction of the truth, prolonging everyone’s misery, and adding 2 million to the Lymie roll-call every year this insanity continues. No more lies. No more patronizing us victims. No more gravy train. Ask them what OspA is. Ask them what it does. I dare you. Ask about the falsified case definition. Ask if they know how to cure post sepsis. Everyone punch them in the gut. Ask them.
_______________________
Follow-up data…
Who else says OspA alone is responsible for this sepsis-then-immunosuppression outcome?
1.) Norman Latov on how OspA vaccination caused the same disease as chronic Lyme:
Neuropathy and cognitive impairment following vaccination with the OspA protein of Borrelia burgdorferi.
“Neurological syndromes that follow vaccination or infection are often attributed to autoimmune mechanisms. We report six patients who developed neuropathy or cognitive impairment, within several days to 2 months, following vaccination with the OspA antigen of Borrelia burgdorferi. Two of the patients developed cognitive impairment, one chronic inflammatory demyelinating polyneuropathy (CIDP), one multifocal motor neuropathy, one both cognitive impairment and CIDP, and one cognitive impairment and sensory axonal neuropathy. The patients with cognitive impairment had T2 hyperintense white matter lesions on magnetic resonance imaging. The similarity between the neurological sequelae observed in the OspA-vaccinated patients and those with chronic Lyme disease suggests a possible role for immune mechanisms in some of the manifestations of chronic Lyme disease that are resistant to antibiotic treatment.” http://www.ncbi.nlm.nih.gov/pubmed/15363064
2.) Gary Wormser on OspA causing immunosuppression (which means it was the opposite of a “vaccine”):
Modulation of lymphocyte proliferative responses by a canine Lyme disease vaccine of recombinant outer surface protein A (OspA).
“… After exposure to either the unaltered vaccine preparation or OspA prepared in saline, normal lymphocyte responses to the mitogens concanavalin A, phytohemagglutinin-M or pokeweed mitogen, or the antigen BCG were consistently reduced. Whole cell extracts of B. burgdorferi also modulated immune responses but required a much greater quantity of protein than needed for theOspA preparation. The magnitude of modulation was directly dependent on the quantity of OspA. OspA interferes with the response of lymphocytes to proliferative stimuli including a blocking of cell cycle phase progression. Future studies designed to delete the particular region or component of theOspA molecule responsible for this effect may lead to improved vaccine preparations.”
http://www.ncbi.nlm.nih.gov/pubmed/10865170
3.) Donald H. Marks – an OspA vaccine trial administrator – on how LYMErix caused the same disease as chronic Lyme:
Neurological complications of vaccination with outer surface protein A (OspA).
”A wide range of neurological complications have been reported via the medical literature and the VAERS system after vaccination with recombinant outer surface protein A (OspA) of Borrelia. To explore this issue, 24 patients reporting neurological adverse events (AE) after vaccination with Lymerix, out of a group of 94 patients reporting adverse events after Lymerix vaccination, were examined for causation. Five reports of cerebral ischemia, two transient Ischemic attacks, five demyelinating events, two optic neuritis, two reports of transverse myelitis, and one non-specific demyelinating condition are evaluated in this paper. Caution is raised on not actively looking for neurologic AE, and for not considering causation when the incidence rate is too low to raise a calculable difference to natural occurrence.”
http://www.ncbi.nlm.nih.gov/pubmed/21673416
4.) Ben Luft at the 1998 FDA Vaccine Meeting on LYMErix:
“The point that I wanted to make in regard to the study is that there is very heavy dependence on serologic confirmation. And when we start thinking about the adverse events, *** it was stated originally when we got the overview of the disease that the disease is really quite protean. And actually the adverse events are very similar to what the disease manifestations are.**** And if you start to, as I think Dr. Hall was eluding to — if you start to kind of say well how often do you actually become seropositive, you can start to have a different take on when someone has an adverse event or whether it is disease specific or infection specific versus vaccine specific. And I think that that is an important issue that we have to deal with. …” http://www.fda.gov/ohrms/dockets/ac/98/transcpt/3422t1.rtf
5.) Dave Persing who together with Yale’s Robert Schoen developed this test in 1994 or 1995 says this about the similarities between Lyme and LYMErix disease:
“Additional uncertainty may arise if the vaccines are not completely protective; vaccinated patients with multisystem complaints characteristic of later presentations of Lyme disease may be difficult to distinguish from patients with vaccine failure….”
Who else says OspA alone is responsible for the immunosuppression with brain inflammation that is characteristic of “Chronic Lyme?”
6.) THE NIH (Martin and Marques):
Borrelia burgdorferi Induces TLR1 and TLR2 in human microglia and peripheral blood monocytes but differentially regulates HLA-class II expression (2006).
The spirochete Borrelia burgdorferi is the agent of Lyme disease, which causes central nervous system manifestations in up to 20% of patients. We investigated the response of human brain microglial cells, glial progenitors, neurons, astrocytes, as well as peripheral blood monocytes to stimulation with B. burgdorferi. We used oligoarrays to detect changes in the expression of genes important for shaping adaptive and innate immune responses. We found that stimulation with B. burgdorferi lysate increased the expression of Toll-like receptors (TLRs) 1 and 2 in all cell types except neurons. However, despite similarities in global gene profiles of monocytes and microglia, only microglial cells responded to the stimulation with a robust increase in HLA-DR, HLA-DQ, and also coexpressed CD11-c, a dendritic cell marker. In contrast, a large number of HLA-related molecules were repressed at both the RNA and the protein levels in stimulated monocytes, whereas secretion of IL-10 and TNF-alpha was strongly induced. These results show that signaling through TLR1/2 in response to B. burgdorferi can elicit opposite immunoregulatory effects in blood and in brain immune cells, which could play a role in the different susceptibility of these compartments to infection.
http://www.ncbi.nlm.nih.gov/pubmed/16783164
The NIH patent explaining how Lyme causes LYMErix-disease (“stealth bomber”):
“The invention relates to novel antigens associated with Borrelia burgdorferi which are exported (or shed) in vivo and whose detection is a means of diagnosing Lyme disease. The antigens are extracellular membrane vesicles and other bioproducts including the major extracellular protein antigen. Another object of the invention is to provide antibodies, monoclonal and/or polyclonal, labeled and/or unlabeled, that are raised against the antigens. A further object of the invention is to provide a method of diagnosing Lyme disease by detecting the antigens in a biological sample taken from a host using the antibodies in conventional immunoassay formats. Another object of the invention is to provide kits, for the diagnosis of Lyme disease, comprising the antibodies and ancillary reagents. The advantage of the antibodies used in the invention is that they react with the antigens from geographically diverse strains of Borrelia burgdorferi, but do not react with antigens from related Borrelia spirochetes.”
http://patft.uspto.gov/netacgi/nph-Parser?Sect1=PTO1&Sect2=HITOFF&d=PALL&p=1&u=%2Fnetahtml%2FPTO%2Fsrchnum.htm&r=1&f=G&l=50&s1=5,217,872.PN.&OS=PN/5,217,872&RS=PN/5,217,872
The shed blebs (or exosomes or vesicles) have LYMErix on them (delayed fuse or “time bomb”):
Characterization of multiprotein complexes of the Borrelia burgdorferi outer membrane vesicles.
“Although we uncovered the existence of at least 10 distinct OM complexes harboring several unique subunits, the complexome is dominated by the frequent occurrence of a limited diversity of membrane proteins, most notably P13, outer surface protein (Osp) A, -B, -C, and -D and Lp6.6.”
http://www.ncbi.nlm.nih.gov/pubmed/21875077
Steere was at the 1994 FDA meeting where Raymond Dattwyler told the FDA Vaccine Committee that the patients with low or no antibodies are the sickest:
“– the ones that (sic) failed to mount a vigrous immune response tended to do worse. So, there is an inverse correlation between the degree of serologic response and the outcome.
“So, individuals with a poor immune response tend to have worse disease.”
See the Occam’s Razor for more.
Categories: Activism, Immunosuppression Diseases, Lyme 101, Lyme Disease
 An Institutional Form of Murder
An Institutional Form of Murder  Lyme Awareness: You Cannot Inject Fungi Into Humans
Lyme Awareness: You Cannot Inject Fungi Into Humans 
Dear Beaux, I read your blogs over and over, at different times, in different days to let it sink in more and more. Eventually, my slow lyme brain will read all your writings posted. I read them not because I do not understand, but because I am SHOCKED at the general denial despite the CLEAR information and the ignorance of the MD’s community.
When I read these I always learn one little bit more valuable information. In this one you said something that sticked with me….. I tested CDC positive for lyme -2 bands- ….after 18 months of treatments (mostly herbals) I am better but not really the way I want to be better. I do more than most people healthy people trying to convince myself that I am not sick…. BUT…. I am still sick.
I quit going to my ID MD in Dec. 2106, we had disagreements and he clearly told me he could not help me any longer. This was the ONLY legit MD the insurance company accepted and he knows how to work that system.
Anyway…..I had a suspicion that I was a lucky one because… I tested CDC positive. I was dealing with lyme for at least 9 months before testing. Maybe more. Definitely, now, looking back at the odd symptoms. It makes sense that I probably did not have lyme as my main infection but BLO which overlapped with lyme. 80% of my symptoms were and still ARE neurological.
I do not have an LLMD, because of financial constrains. I could not afford one and I felt the same way you described in your post. I wanted run away from these MD….ND….who are taking advantage of people illness misery. So here I am, alone, treating to manage this crappy immunosuppressant disease. It killed me in the money department. Above all it killed my dreams and motivation to live life I had before lyme.
I tried many things including prescribing my own antibiotics when I felt it was necessary. I am not holding my breath hoping for any scientist, researcher or MD to help me get better in this life.
However I thank people like you Beaux who are enlightening my path. “Enlightening” it seems inappropriate term for such not-hope disease. Fungal disease makes so much sense to me and explains why some herbal treatments are better than antibiotics for some of us because of fungicide properties and immune system remodulation. I feel that any ILADS MD are somewhat a bunch of opportunistic professionals who found a way to the golden wealth well.
Thank You again.
LikeLike
___123___The Lyme Gut Punch___123___
LikeLike
Best course of treatment to feel better long term and short term? IVIG, antivirals, antibiotics, Immune modulation herbs? Vitamin supplementation?
LikeLike
As I am not a licensed medical professional, I can only explain the disease mechanisms–not how to treat. Unfortunately we don’t have any licensed medical professionals who care to read the science. That puts us all in a bit of a bind! Anything that’s available to us right now is just a Band-aid, and it’s up to each individual to find some relief through trial and error. I’ve done 3 IVIGs and so far, zilch.
LikeLike
yes but we have learned so much about healing that big pharmacy is starting to become a last option for those listening. The more they hide things the more others seek help elsewhere the more common natural healing is becoming. Either way they lose. They have no good way out.
LikeLike
I’m an artist, not a scientist, but think I understand what you’re saying. Those of us with chronic Lyme are actually dealing with an acquired immune deficiency, which re-activates viruses like EBV. This would help explain the debilitating chronic fatigue that keeps us from being able to participate in normal life.
LikeLiked by 1 person
Yes, that’s exactly right. More people need to understand that so we can get the validation and treatment we so badly need and deserve. I’m not a scientist, either.
LikeLike
I’m just starting to understand this, it has taken me a while to get my head around it, and it is so interesting.
I tested positive through a German lab for Borrelia on only one of their Borrelia tests- OSPA/OSPC/DbpA but negative for other tests and IgG and IgM. Also positive for EBV and Coxsackie.
These results seem to fit the picture that you are talking about.
Thanks for the blog.
LikeLike
Thoughtful. But could we be looking at immunosuppression AND residual bacteria? Could explain why patients still respond to antibiotics but never get fully well.
LikeLike
It’s mainly the opportunistics to which we become tolerized, that the antibiotics are treating. Spirochetes go to the brain, lymph nodes and bone marrow, and hang out with the EBV.
LikeLike
Would this also explain the lower body temperature experienced by chronic Lyme sufferers?
LikeLike
Reblogged this on Lyfe and commented:
Thanks again. Beaux. I just keep reading and reading. Hopefully at some point some of this will find it’s way into my brain… A gal can hope.
LikeLiked by 1 person
One day it will all click and you’ll be astounded.
LikeLike
I’m already well into astounded! Part of me wants to scream WHAT SHOULD I DO at you but I know that’s not fair… My family is so profoundly affected by this bullshit I can barely breathe. Looking to make a deal with the devil at this point. If he can make my 16 year old stop seizing and be free of that damn wheelchair… I’d gladly give him whatever he asks in return. My soul, my left arm… Whatever.
LikeLiked by 1 person
I know. I’m so sorry. As parents we really would do literally anything. 😞
LikeLiked by 1 person
so, we dont have LYME DISEASE, IS THAT WHAT YOUR SAYING? I DONT UNDERSTAND!!! then what do we have and what is the difference anyway..just a different name, but still the same symptons? im really confused. so we are treating for the wrong illness? what do we tell our mds ? what do i have now!
LikeLike
What if we never had the vaccine, I have been bitten by ticks as a child in the South and also as an adult in NC, but the doctor that diagnosed me said I got it congenitally in the womb??? Can you give me context as to how I got tick shit sepsis?
LikeLike
No need for the vaccine. The vaccine was OspA, which is the shit sepsis toxin that is on the shed borrelial blebs.
LikeLike
so what do we have..is it bacterial, and cos or what..i was nerver good in biology…..please, in lay terms whhat the hell do we have…i never got the vacine. ie had this for 28 yrs…what am i treating..maybe i should quit trying?
LikeLike
Look up post sepsis syndrome. It’s an acquired immune deficiency. We become susceptible to all kinds of infections which is why antibiotics seem to work sometimes, but because of the immune deficiency they keep coming back. Also latent herpes viruses like Epstein Barr and CMV get chronically reactivated.
LikeLike
Wowwwww! This changes everything!! I am not CDC POSITIVE because I don’t have antibodies, they gave up a long time ago 😥 ! In-freaking-credible!!! I am IGeneX positive, been bedridden since 2012! They’ve known all along what is wrong with us, this makes it 1,000 X’s worse for me 😥 …. THANK YOU FOR THE TRUTH!!!!!!!!!!
LikeLiked by 1 person
This info is really interesting and I really appreciate you for putting it out there in an easily digestible manner. I know you are mostly about activism with the Dearborn case, but reading this fills me with dread as what to do. I know that you are not a doctor, but what do you propose for this post-sepsis immunosuppression? IVIG or something else? I know that science is not there yet, but those of us have to do something. We have to find the right doctors. What advice do you have for treatment?
LikeLike
A mechanism such as this driving chronic Lyme is something I’ve long suspected given the present outcomes of diagnosis and treatment under whichever major Lyme ideology one picks. It does jibe with my own experience and observations.
The big question is, what can one practically do with this information in regards to treatment? I’ve long accepted no MD’s in either camp have any sort of a handle on this thing. For me, for years it has been personal trial and error to work out a regimen that keeps me functional most of the time. I suspect it is the same for many who refuse to stop thinking and stop fighting. After a period of time with a poorly defined and treated illness, many of us are financially crippled and can not afford medical expenses not sanctioned by our insurers.
LikeLike
What we are trying to do is get the fraud and RICO prosecuted, and the falsified case definition thrown out so people can at least start getting diagnosed and getting disability. Until there is recognition of the true disease mechanism, we’ll still be grasping at straws to find the most basic symptom relief. We simply must get Dearborn out of the way and all the bogus research retracted.
LikeLike
TO: Beaux Reliosis–This makes a lot of sense. Given the reality of the situation, what is our action plan? What kinds of research needs to happen to help patients?
LikeLike
We need acknowledgement that this is a disease of immunosuppression for most people (There are plenty of scientists who say so already, including the crooks) and that the case definition was falsified to identify only the 15% hypersensitivity cases. It always goes back to exposing the fraud of the Dearborn conference. We are currently working on a video that will explain how Dearborn went down, and what the disease really is. We were advised last year by a staffer of the then-head of the Senate Judiciary Committee that we need to lobby for a hearing to force the DOJ to prosecute.
LikeLike
This is an astounding post, that’s my best description. It’s a concept I have not come across in all my Lyme Ed thus far. Really mind blowing. No spirochetes, no biofilms, no bugs to kill. Both enlightening and frightening all at the same moment. Obviously you put a lot of work into this article. Thank you.
LikeLiked by 1 person
YES! Thank you!!! That’s exactly what we want to hear. I appreciate the feedback very much.
LikeLike
I am very confused. I have Kyme and numerous other autoimmune diseases, viruses, etc. Are you saying that we have to have had these specific vaccines in order to acquire what we think of as Lyme? I for ine have never had these vaccines and neither haas anyone else I asked about this. Could they be hiding it in other vaccines or things like tetanus shots? I had a tetanus shot a few years before I became sick, but no vaccines. Thanks.
LikeLike
Hi Kirstin,
No it’s not in other vaccines, and no, you didn’t have to get the Lyme vaccine to be sick. LYMErix caused the same disease as what we commonly call “chronic Lyme.” What that tells us is that the disease is alone caused by OspA, which was the vaccine antigen, and is just one of the immunogenic parts of relapsing fever spirochetes. OspA is all you need to be sick with “chronic Lyme.” And what does OspA do? It shuts off the immune system so you end up with immune deficiency. Most people do, anyway. 15% have the arthritis haplotypes and get an arthritic knee–those are the autoimmune cases–the ones who produce enough antibodies to test CDC-positive. The CDC dumped the other 85% of us (the sickest, AIDS-like cases) from the disease definition (meaning they changed the diagnostic standard so we wouldn’t test positive) because in the vaccine trials LYMErix was causing “chronic Lyme”-like adverse events, and they opted to protect their profits.
LikeLike
I’m sorry, I’m confused as well. I’ve never had the LymeRx vaccine. Where else would we get ospA from? I’m not quite understanding what you’re saying is causing chronic Lyme or how we heal now.
LikeLike
Spirochetes shed OspA as if stealth bombing your immune system. I’d doesn’t matter if you get OspA injected by an infected tick or through every a syringe.
LikeLike
OspA is OspA. It is the same thing, and has the same effect no matter which way it is administered. They knew this during the LYMErix (OspA) vaccine trials, and that is why they changed the disease definition at Dearborn: to exclude the immunosuppression cases.
LikeLike
Does that help?
LikeLike
Kristen,
Tick’s can transmit OspA to you. They are saying that the tick bite did cause your illness. But it is not Lyme disease. Instead, it is an Aids-like disease. It took me awhile to understand this too.
LikeLike
Wonderful! Just what I needed. The truth!
LikeLiked by 1 person