
One problem all of us abused groups have is that we all tend to focus on our own personal narrative, rather than look at what we have in common. As a victim of chronic Lyme abuse, if I say anything about Myalgic Encephalomyelitis (M.E.) I am immediately perceived as attacking the M.E. crowd. Fingers shoot into the ears and the “la la la la las” shoot out of the mouths. I have news for you: the same thing happens in my Lyme groups, Lymie on Lymie! Very few people want to hear what I (along with ActionLyme, Ohio ActionLyme and CrymeDisease.com) am saying. I dare you, right now, to remove fingers from ears and listen up, because the science tells us that what unites us all is Chronic Sepsis or Post-sepsis Syndrome.
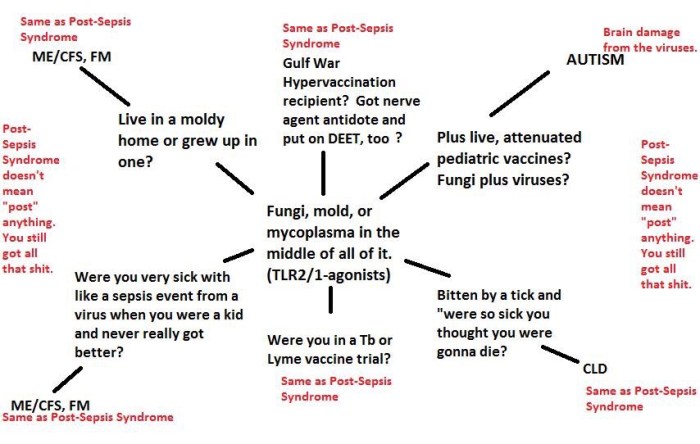
Take a look at this graphic. What it illustrates is that TLR2/1 agonists, at the center of all medically abused groups, provide the mechanism for nearly all chronic illnesses for which cures are denied by the government and medical establishment.
Scroll down here to the list of TLR2 agonists. There’s your OspA, your mycoplasma, your CMV (a herpesvirus), your candida, among many others. Now, remember what I’ve said before about OspA, how it causes immunosuppression and reactivation of those nasty herpesviruses In Lyme disease. All of those TLR2-agonists function in the same way. Yes, mycoplasma, candida and OspA do the same thing. This model of immunosuppression has been known since the 1950s, and has been repeatedly validated in the years since.
See here for Lyme Cryminal Dattwyler talking about a “blunted” immune response, AKA immunosuppression.
The NIH agrees with this model. We are talking about TLR-2 agonists–fungal antigens–which turn off the immune system to prevent death from sepsis and reactivate herpesviruses, whose chronicity have been widely proven as leading to cancers and neurological diseases.
NIH: profound immunosuppression is one of the chronic consequences of severe sepsis
Washington University in St. Louis: Reactivation of multiple viruses in patients with sepsis
NIH: Chronic active EBV disease (CAEBV) is a lymphoproliferative disorder
University of Michigan: The chronic consequences of severe sepsis
NIH saying medical students are *allowed* to have chronic fatigue/reactivated herpesviruses but the rest of us suckers are useless wastes of healthcare, social services and air.
Now can you see what they have done to divide us? They take our varied symptoms and use them to dump us into these different buckets, even though we all are suffering from a trashed immune system, chronic viruses, that toxic fungal-viral-bacterial soup, and all of the cancerous and neurological consequences.
As long as we are divided, money will continue to be thrown at non-curative, symptom-hiding and “psychological” treatments that do not address the root cause of all our suffering: the trashed immune system, or chronic sepsis, or post-sepsis syndrome. (And by the way, there is nothing “post” about it, really, because this immune system damage is permanent and ongoing.)
Now, if you have M.E./CFS or some variation, and you’re still with me, here is how you nail the government crooks who deny your disease and bash you as a mental case or malingerer:
“Blood was collected in sodium citrate Vacutainer tubes (Beckton Dickinson) and shipped by overnight courier to the Centers for Disease Control (CDC), where plasma was collected by separation on lymphocyte separation medium (LSM; ICN Biomedicals). Plasma (1 ml) was concentrated to approximately 250 μl in a Centricon centrifugal filter unit YM-100 (Millipore). Cell-free plasma DNA was extracted by using a QIAamp DNA Mini kit (Qiagen) according to the manufacturer’s instructions and quantified by using a DyNA Quant 200 fluorometer (Amersham Biosciences).”
Categories: Activism, Beaux's Favorites, Immunosuppression Diseases, Lyme Disease
 An Institutional Form of Murder
An Institutional Form of Murder 
Forgot to mention the mycoplasmas causing permeability issues with red blood cells where Oxygen cannot cross the RBC wall, hence, fatigue because of low oxygen. Couple that with the reactivation of EBV and you get the extreme fatigue. Fatigue that will not show up because you still have high/normal RBC count, but not anemia.
LikeLiked by 2 people
Thank you! I’ve made that edit. 🙂
LikeLike
Also, if it’s more of a chronic sepsis than a “post sepsis,” then wouldn’t antibiotics plus fluids actually still be useful? Or an exchange transfusion?? What about using over-the-counter phenylephrine as a vasopressor? (it’s in common decongestents): http://forums.studentdoctor.net/threads/why-not-use-phenylephrine-all-the-time.1000636/ — or all of the above? I also wonder if this is why hyperbaric treatments work in some patients, i.e. that they are treating a septic state that hasn’t progressed beyond repair, since HBOT has shown some efficacy in sepsis.
LikeLike
Hey! This is my first visit to your blog!
We are a team of volunteers and starting a new project in a community in the same niche.
Your blog provided us beneficial information to
work on. You have done a wonderful job!
LikeLiked by 2 people
Thank you very much! Glad to be of help.
LikeLike
Some antibiotics are being found to have anti-cancer effects though, so what about that?
LikeLike
Yes indeed
Lyme is associated with many cancers
Bacterial infecions are found in most if not all cancers
LikeLiked by 2 people
I *currently* have all of the symptoms of severe sepsis, such as blood pressure that rarely gets as high as 90/60 and often is in the 70s/40s, low body temp, etc. That degree of low blood pressure only started when I went into full-blown septic shock from TBDs and nearly died. I haven’t ever recovered. The question is, what does one do then? Would an IV antibiotic plus IV antiviral plus potent antifungal regimen do something? Also, agreed about Vernon, but Nicolson found mycoplasmal involvement decades ago and did treat many successfully w/ antibiotic combinations.
LikeLike
Hello, and thanks for reading! I’m sorry for your struggles. I keep hearing more and more stories from people who either died from the initial septic shock of TBDs or barely made it out alive. I just hate this. If you are having chronic problems after a tick bite, it’s likely that the OspA from borreliae or another fungal antigen turned off your TLR2s, which is permanent, as long as the disease is denied and they aren’t looking for ways to reboot the immune system. Chronic exposure to fungal antigens will do that, causing the immunosuppression, reactivation of herpesviruses and susceptibility to opportunistic infections. Mycoplasma can do that too. I suppose it’s possible Dr. Nicolson’s patients did not yet have permanently damaged immune systems. I see “LLMDs” now treating with combinations of antibiotics/antivirals/antifungals, so it seems they know what’s going on. I even have prescriptions for all of the above, but only take them when things get out of balance. They might help you feel better for a while, but the nature of relapsing fever borreliosis is relapse…and that’s due to the unkillable spirochetes constantly blebbing their OspA. The thing to keep in mind is that diseases of immunosuppression are in the cancer class–not the autoimmune class, as IDSA would have us believe. So, there is potential for certain cancer therapies to help us, if only we can get this whole thing out in the open and treat what’s really going on.
LikeLiked by 1 person
Antibiotics-hold off because there will be a day you HAVE TO HAVE THEM and they wont work-KNOW YOUR BODY-READ-BE YOUR OWN DOCTOR-AND-I HAVE NEVER SEEN A DIVISION BETWEEN US-MAYBE DIFFERENT IDEAS! We all agree WE WON’T GO ANOTHER 40 YEARS!
LikeLike
Reblogged this on keuninckx.
LikeLiked by 2 people
Thank you for sharing!
LikeLike
I am fixing to reblog the same way 🙂
LikeLiked by 1 person
Reblogged this on The Other Side Of The Stretcher and commented:
Did You Know This?
Call Dr Anthony Fauci at the NIH and ask him about it!
LikeLiked by 4 people
What a bunch of creeps! I did not know this!
LikeLiked by 1 person
Yes! Maybe I’ll start devoting a post to the dirty deeds of every creep. 😉
LikeLiked by 1 person
Lets start The world to know… Greetings from Norway. Norway start to wake up- halo USA!!
LikeLiked by 2 people